Date: March 7, 2000
Interstitial Cystitis Network - Chat Log (www.ic-network.com)
Topic: SANS - Stoller Afferent Nerve Stimulation for Frequency, Urgency and
Incontinence
Speaker: Dr. Marshall Stoller, UCSF
![]() We
would like to thank our sponsor, AKPharma
(makers of Prelief), for helping to make this, and other ICN chat events,
possible during the year 2000. Our corporate sponsors help us to maintain
the largest free archive of IC information in the world, now accessed by patients
and providers in 69 countries.
We
would like to thank our sponsor, AKPharma
(makers of Prelief), for helping to make this, and other ICN chat events,
possible during the year 2000. Our corporate sponsors help us to maintain
the largest free archive of IC information in the world, now accessed by patients
and providers in 69 countries.
<icnmgrjill> Greetings everyone. Tonight we welcome Dr. Marshall Stoller of the University of California San Francisco (UCSF) Medical Center. Dr. Stoller is one of the most popular urologists on the west coast, not only for his reputation as a very fine surgeon, but also his compassion for IC patients. I saw him as a patient back in 1993 and it was such a relief to walk into a room with a physician who believed everything that I said and who believed that I was in such pain. Many things have happened since then and Dr. Stoller finds himself at the forefront of an exciting new development in the urology community, the recent FDA approval of his SANS unit (Urosurge). Dr. Stoller, welcome to the IC Network.
<drstoller2> It's an honor to be here with you.
--------------------Presentation Begins---------------------
<icnmgrjill> Dr. Stoller, can you tell us how you first got interested in treating IC patients?
<drstoller2> As a surgeon, I take care of a lot of pathology that you can see and feel. The IC patient represents a patient that has a functional disorder. You can't see a mass. You don't have an infection. Most urologists consider themselves surgeons. However, in a typical urologists office only 30% of these patients require surgery. Seventy percent of the patients that come through our offices have functional disorders and there is a need to address these patients. IC patients have real problems requiring real solutions.
<drstoller2> One of my most memorable patients with IC was shuttled from doctor to doctor. She had had multiple operations. She had her uterus and ovaries taken out. She had her appendix taken out. She had her gall bladder taken out. And I remember this patient as someone with pelvic pain without pelvic organs, because the people that she sought to help were surgeons. Their mindset was an honest effort to remove the problem. I recognized that IC, like other functional disorders, could not be routinely addressed by removing organs. It was at that time that I put my mind forward to find a minimally invasive treatment approach to help these large numbers of patients.

<icnmgrjill> What is SANS?
<drstoller2> Stoller Afferent Nerve Stimulation (SANS) is a new approach to the clinically proven technique of electrical stimulation for the treatment of urge incontinence syndrome. The device consists of an electrical generator (like a TENS unit), a cable with grounding pad, and a 34 gauge needle.
<icnmgrjill> Why does SANS work?
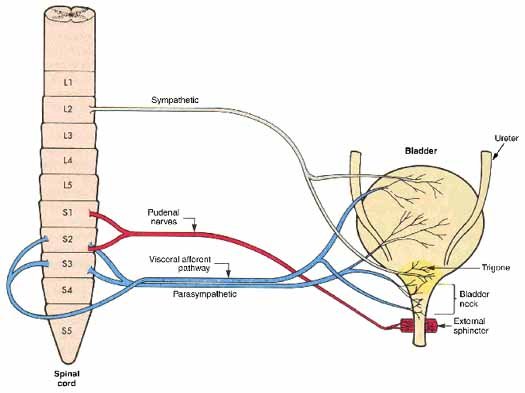
<drstoller2> Studies have shown that the S3 region of the spinal cord plays a key role in the neurologic control of bladder function. Electrical stimulation, using electrodes implanted in near S3, has been shown to be effective in treating urge incontinence and it's associated conditions. The SANS device is a less invasive method of gaining access to the S3 junction of the spine, so that patients would not have to endure invasive surgery. SANS stimulates the nerve from the ankle, rather than through an invasive spinal procedure.
<icnmgrjill> Why would neuromodulation work?
<drstoller2> There are a lot of things that we do not understand in medicine. A good example is when someone has lack of blood to their heart when they are having a heart attack. Sometimes there is pain that radiates from their heart to their left arm and up to their jaw. Yet, there are no nerves that go from the heart to the arm.. or the heart to the jaw. But these symptoms are real. When there is lack of blood to the heart, some people get severe pain called angina. Some people get a funny rhythm of the heart. These, at times, can be deadly.
<drstoller2> An analogous situation can be seen in the pelvic floor. Some people experience severe pain and some people experience marked urinary frequency. Some people experience urinary urgency or urge incontinence. Many people experience a little of each one of these.
<drstoller2> To study potential lack of blood flow to the pelvis, I had five adult male patients who were impotent more than five years each. They had no erections and they had no tumescence to the penis. The same blood that goes to the bladder and to the pelvic floor goes to the penis. It was a unique opportunity to understand the role of blood flow in pelvic floor dysfunction.
<drstoller2> These patients were placed in a quiet examining room for 20 minutes. An objective urologist utilized Doppler ultrasound to assess penile blood flow. We then repeated these studies twenty minutes later. We then placed and activated a SANS stimulator in the lower leg and then rechecked the blood flow. Remember, these patients get no erections. Remarkably, after SANS stimulation, blood flow to the penis increased 80%. For me, this was exciting information to help understand how peripheral nerve stimulation can have a dramatic life changing impact on patients.
<drstoller2> The pelvic floor is a unique part of the body. It has the input from two neural networks. The first is the somatic input where we have voluntary control.. we lift our arm.. we lower our arm. When you have the urge to void, you can successfully inhibit that urge by voluntarily contracting the pelvic floor. The urge will frequently come back 15 or 20 minutes later.
<drstoller2> Additionally, there is input from the autonomic nervous system. These are involuntary nerves that control bladder contractions, similar to other smooth muscles in the body. The pelvis is the only location of the body where there is input from both the somatic and autonomic nerves.
<drstoller2> Peripheral nerve stimulation likely balances these two neural networks and help to increase blood flow in the pelvis. This is why these peoples lives are dramatically changed.
<icnmgrjill> How is it done?
<drstoller2> Of the nerves that emanate from the S3 junction in the spine, the posterior tibial nerve runs all the way down the leg to the foot, where it is close to the surface of the skin and easily accessible. We place a 34G (standard acupuncture) needle through the skin and near the nerve. We then attach a small electrical stimulator to the needle to deliver the electrical current directly to the location of the posterior tibial nerve. The impulse is then conducted via the afferents (nerves that send messages from the periphery of the body back towards the spine, rather than from the spine to the limbs) of the tibial nerve back up the leg to the S3 junction at the spine, producing the neuromodulation effect.
<icnmgrjill> What are the advantages of SANS over other procedures?
<drstoller2> The SANS device offers patients relief from the incapacitating conditions associated with urge incontinence syndrome, without the problems associated with current forms of treatment.
<drstoller2> (1) SANS does not require vaginal or rectal probes which
can be uncomfortable or painful.
<drstoller2> (2) SANS has none of the side effects seen with medication.
<drstoller2> (3) SANS is a simple, cost effective office based procedure.
<drstoller2> (4) SANS is a non surgical solution thus, eliminating the
complications associated with surgically implanted stimulators
<icnmgrjill> How often does a patient use SANS? Is more better?
<drstoller2> We have patients come in once a week, for 30 minute sessions. This will occur over a 10-12 week period, after which the patients response is evaluated. If the patient is responding well, the frequency of treatments is slowly reduced to minimize the number of visits while still maintaining the positive benefits of the therapy. Treatment frequency may range from once per week to once every two months.
<icnmgrjill> What results did the clinical trials have?
<drstoller2> The SANS device was evaluated for the treatment of patients with pelvic floor dysfunction with symptoms of urinary frequency, urgency or urge incontinence in a single investigator study and a corroborative 12-week study. We treated approximately 100 patients with the SANS device and are seeing an approximate 80% success rate in treating urge incontinence syndrome, including urgency and frequency.
<drstoller2> A total of 63 patients received SANS treatment in the corroborative study. In the corroborative study, 71% of patients were classified by the investigators as a treatment success.
<icnmgrjill> Thank you Dr. Stoller. Let me just say we'll be publishing the list of national researchers tonight. They are located throughout the US.
--------------------Q&A Begins---------------------
<icnmgrjill> Let's go ahead and take some Q&A. If you have a question for Dr. Stoller, please whisper it to Lesa or Terri or myself and we'll put you in the queue. Tracee has the first question. She wants to know if it helps with pain?
<drstoller2> The device was approved for frequency and urgency by the FDA. However, I have had good experience in patients with severe pelvic pain.
<icnmgrjill> Speaking as one of those patients, it certainly helped to reduce my pain back in 1993. I'll be happy to describe my experience with SANS by e-mail with anyone. You can reach me at: jill@sonic.net.
<icnmgrjill> Our next question is from Ann. She wants to know if SANS can effect S3 and S4 at the same time?
<drstoller2> Afferent nerve stimulation directs the stimulus towards the spinal cord whereas efferent stimulation, like Interstim, stimulates the nerves as they exit the spinal cord. With the afferent nerve stimulation of SANS, you are not as specific in stimulating S3 or S4. However, I believe that afferent nerve stimulation will, hopefully, balance the output from the spinal cord in alleviating the pelvic floor dysfunction.
<icnmgrjill> Our next question is from Mary. She wants to know which symptoms do you feel that SANS would address in order of efficacy? frequency? pain? urgency?
<drstoller2> I think that the symptom most readily treated is urinary frequency, then urgency and urge incontinence and then pain. It is important to remember that individual patients can have tremendous overlaps in these symptoms and that when one improves, it is frequently found that the others will quickly follow.
<icnmgrjill> Our next question is from Bev. She has a question about hypersensitivity. She says that IC patients, as well as patients with IBS, appear to develop hypersensitive nerves and become sensitive to stimulation of those nerves. Does that relate, in some way, to how SANS works or does not work?
<drstoller2> The best way for me to answer this question is to give an example of someone walking into a coffee table and hitting their shin on a corner. The natural response is to rub the area of injury. Why? For most people, this additional stimulation alleviates and eases the pain. In a similar fashion, SANS technology can increase neural input to ease the neural output, whether it be pain.. frequency or urgency. Some people refer to this as the gate theory. This is a part.. but not complete answer.. of how this may work.
<icnmgrjill> Are their are any side effects to SANS?
<drstoller2> We have seen no significant side effects to SANS. When the needle is inserted, there may be some pain if the needle hits surrounding bone. The needle is then easily readjusted. There is no prolonged pain. I've been doing this for well over ten years and have not had any infection or severe side effects.
<icnmgrjill> Suzanne asks "If this is more effective than some other strategies, then why isn't this a first line approach to treating IC?"
<drstoller2> I believe that this is a potential first line of approach for pelvic floor dysfunction including those with pelvic pain, frequency, urgency and urge incontinence. It doesn't conflict with other treatments, nor does it preclude other treatments in the future. The hardest part right now is letting those physicians and patients know that this is a viable first line therapy. It's affordable and accessible.
<icnmgrjill> SI wants to know if this is something that can be done at home by the patient?
<drstoller2> The FDA has not approved home therapy yet, however, I have treated many patients initially at the office and had them placed the needles with stimulation for many years. This increases freedom for the patient and I believe the patient cannot hurt themselves by placing the needles in the ankles. It is not like placing a needle in the neck or other vital areas in the body.
<icnmgrjill> Dr. Stoller taught me how to do this at home several years ago and I've found it to be amazingly easy to do. It takes about 30 minutes and eliminated my need to drive 2 hours to see him, which was very difficult back then.
<icnmgrjill> Our next question is from Sue. She wants to know how you work with patients who are terrified of needles?
<drstoller2> I used to be terrified of needles and I am now a surgeon. I think that fear is mainly due to the unknown. It isn't painful placing the needle and many patients that I have close their eyes when I put it in. I feel as long as their is a reasonable relationship between the patient and doctor, that placing the needles isn't a problem. I've taught elementary school and junior high school children to place their own needles. When these children saw their results and when these children were not made fun of anymore by their peers, placing the needle became even easier.
<icnmgrjill> I can hear his beeper going off right now, so let's let Dr. Stoller go. Thank you Dr. Stoller. We so appreciate your time!
<drstoller2> I will be happy to come back at a future time with Jill and others to answer any other questions. I want to offer you hope that this process is not a cure all but, for a substantial number of patients, it will significantly offer the quality of their lives.
-------------------- Clinics Participating in SANS Research --------------------
California
Marshall Stoller, M.D.
University of California San Francisco
Department of Urology
533 Parnassus Ave
San Francisco, CA 94143-0738
(415) 476-1611
Iowa
Karl J. Kreder, Jr., M.D.
University of Iowa Hospitals and Clinics
Department of Urology
200 Hawkins Drive
Iowa City, IA 52242
319-356-0748
Massachusetts
Peter Rosenblatt, M.D.
Mt. Auburn Hospital
300 Mt. Auburn Street
Suite 302
Cambridge, MA 02138
617-354-5452
New York
Victor Nitti, M.D.
New York University Medical Center
Department of Urology
540 First Avenue, Suite 10U
NY, NY 10016
212-263-6301
Alan Garely, M.D.
North Shore Women's Health
Long Island Jewish Health System
865 Northern Boulevard, Suite 202
Great Neck NY 11021
(516) 622-5114
Ohio
Rodney A. Appell, M.D.
Head, Section of Voiding Dysfunction and Female Urology
Department of Urology - A100
9500 Euclid Avenue
Cleveland, Ohio 44195
800-223-2273, x44662
Oklahoma
Scott Litwiller, M.D.
Urologic Specialists of Oklahoma
Warren Professional Bldg.
6465 S. Yale, Suite 704
Tulsa OK 74136
918-491-5700
Washington State
Fred Govier, M.D.
Virginia Mason Medical Center
Department of Urology
1100 Ninth Avenue
P.O. Box 9000
Seattle, WA 98101
206-223-6772
Wyoming
Stacy J. Childs, M.D.
Cheyenne Urological, P.C.
800 East 20th Street
Suite 101
Cheyenne, WY 82001
307-635-4131
----------- After the Chat & Announcements ------------
<icnmgrjill> Dr. Stoller is truly one of the nice guys. He was in the Operating Room all day today and still came to chat with us. His beeper was going off for the last twenty minutes and he stayed to take your questions. That was very nice of him.
<HelenB> Jill - did you have a home unit for this?
<icnmgrjill> Helen.. I sure do. Of the treatments that I've done, this was the easiest and certainly one of the most effective. My IC had just started and I was so ill back then. I was in a lot of pain when I first saw him. At week 4 of the procedure, I had my first 2 hours without pain and no flare before my period, which was a subtle sign of improvement. At week seven, I had my first day without pain. He was the first doc to really give me hope!
<HelenB> What "type" of doctor is Dr.Stoller pain management, urologist?
<icnmgrjill> He's a urologist at University of California San Francisco Medical Center and a highly respected surgeon.
<icnmgrjill> Oh, by the way, two announcements.
(1)In the news today, they released a story of a young toddler who died after taking megavitamins and minerals. He was under the care of a nutritionist but his mother didn't think that the vitamins and mineerals were making a difference so, on her own, she upped the dosage 300%. He had magnesium poisoning. This is just one more important message for IC patients because we should not self medicate like this. There are definitely risks to those alternatives.
(2) The FDA released a position paper on colloidal silver last year that I just found. It says that "over the counter drug products containing colloidal silver ingredients or silver salts are not generally recognized as safe and effective and are misbranded. The FDA is issuing this final rule because many OTC drug products containing colloidal silver are being marketing for numerous serious diseases.. and the FDA has found no scientific evidence which supports their use." So for those of you who had considered colloidal silver for your IC, you should absolutely be aware that the FDA is saying, once and for all, that this is dangerous and that there is no scientific evidence that it can be helpful.
Please review the ICN Disclaimer: Active and informed IC patients understand implicitly that no patient, or web site or presentation on a web site should be considered medical advice in all cases, we strongly encourage you to discuss your medical care and treatments with a trusted medical care provider. A copy of our more extensive disclaimer can be found at: http://www.ic-network.com/disclaimer.html
The opinion of the speaker is not necessarily the opinion of the IC Network.
Copyright © 2000, The IC Network, All rights reserved. This transcript may be reproduced for personal use only. If you do so reproduce, we ask only that you give credit to the source, the IC Network, and speakers, Marshall Stoller and Jill Osborne. For additional use, please contact the ICN at (707)538-9442.